Your Living Action Plan
A friendly map of where your health stands today, what your care team is watching, and the questions most useful to bring to your next visit.
How to use this plan
Welcome. Think of this plan as a place to get oriented, feel prepared, and ask better questions. It is built from your medical records and a careful review of your case.
This plan supports the conversations you have with your doctors. It does not change your care on its own, and it does not replace your care team. Grace, your CaringHand companion, can walk through any part of it with you, in plain language, whenever you want.
Early-stage colon cancer, fully removed
Because it was found early and removed completely, you did not need chemotherapy or radiation. Your recent cancer check-ins have been reassuring. Alongside your cancer follow-up, your team also keeps an eye on your blood counts, blood sugar, and heart-and-metabolism numbers.
The milestones that brought you here
A simple picture of your colon
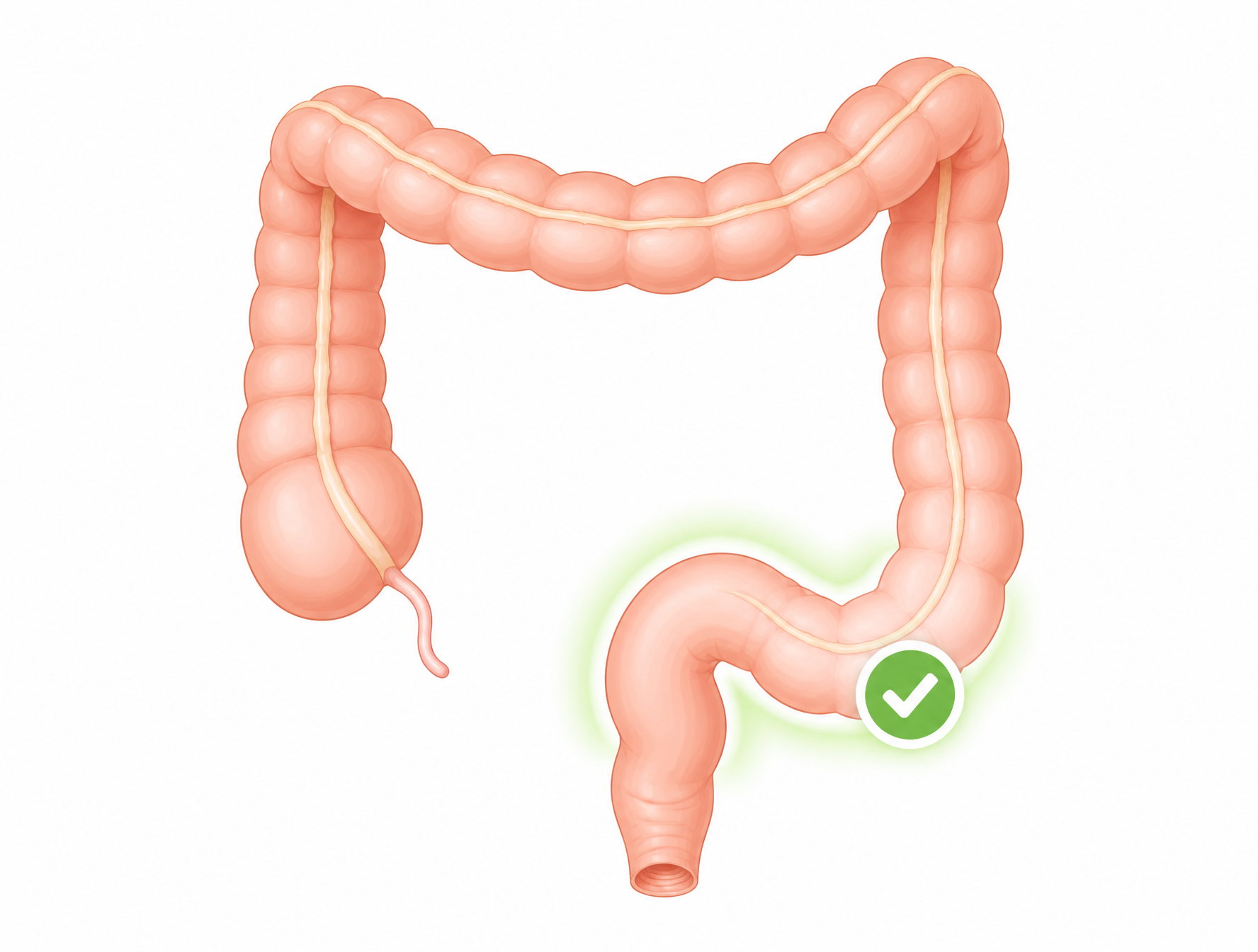
Your colon is your large intestine. The lower S-shaped part is called the sigmoid colon. That is where the early cancer was found and fully removed, shown here with a green check.
The rest of your colon is watched too, because it tends to form polyps. This picture is just for orientation. It does not show any active disease today.
Areas being kept an eye on
This is a "watching" list, not a "to-do" list. Your care team decides what to check and when, together with you.
Your colon
Blood counts & B12 Likely next
Your blood sugar
Heart & metabolism
Your calcium
Your sleep breathing
What gets checked, and about how often
This is the general rhythm your care team uses to stay ahead of things. Exact timing is always set by your team, with you.
| What | About how often | Why it helps |
|---|---|---|
| Colonoscopy | Next later in 2026, then about every 1 to 3 years | The main way to find and remove new polyps early, given your polyp history. |
| CEA blood marker | At routine oncology visits | A simple blood signal followed over time. Yours has stayed steady. |
| Oncology survivorship visit | About once a year | A regular check-in on the whole picture. |
| Blood counts and B12 | As your team advises while this is looked into | To understand the rising hemoglobin and high B12. |
| Blood sugar and metabolic labs | Through your primary care and diabetes visits | To track and fine-tune these numbers over time. |
| Routine CT scans | Not a routine part of your plan right now | For an early-stage cancer that was fully removed, routine scans are usually not advised. Your team decides if a scan is ever needed. |
This is a general picture, not an appointment list. Your care team confirms each date with you.
The pieces work together
Your care team looks at the whole picture, because several areas of health are linked. Supporting one often helps the others.
This is a simplified picture to help conversations, not a diagnosis. Your care team interprets what it means for you.
Two numbers over time
These charts simply show two trends. Your care team is the one who interprets what they mean for you.
Hemoglobin (oxygen-carrying blood)
What is known: this number has slowly risen above the usual range over about two years. The cause is what your team would like to look into, likely with a blood specialist.
A1c (average blood sugar)
What is known: this number improved, then crept back up over recent months even on strong medicine. A metabolism specialist is someone who could help fine-tune things.
Steady supports for everyday life
Think of these as anchors, not rules. Small, consistent habits add up.
Movement
Eating
Hydration
Sleep
Weight & metabolic
Alcohol
Why activity is one of your strongest tools
Staying active does more than help your weight. A mix of walking and gentle strength work supports your blood sugar, your heart, your mood, and your muscle, all at once.
For colon health over the long run, staying active and keeping muscle are thought to be supportive. You already exercise regularly, which is a real strength to build on.
This explains general supports. It is not a prescription. Your care team can help you shape activity safely.
Helpful for screening conversations
Organizing your family history makes it easier to discuss what screening, if any, makes sense for you.
A maternal grandfather also had an unknown cancer at an older age. A good question for a visit: given this history, are there other screenings worth planning, and would testing your original tissue sample help?
Whole-body scans and multi-cancer blood tests
Some people ask about extra tests they have seen advertised, like a whole-body MRI scan or a multi-cancer early detection (MCED) blood test (for example, the kind marketed under names like Galleri). Here is a balanced way to think about them, to discuss with your care team.
Whole-body MRI
It is a scan with no radiation that looks broadly across the body, which some people find reassuring.
For an early-stage cancer that was fully removed, broad scans are not a standard part of follow-up. They often turn up harmless spots that lead to more tests and worry.
MCED blood test (for example, Galleri)
It is a single blood draw that aims to look for signals from several cancers at once.
These tests are newer and are not yet a standard or guideline-recommended part of survivorship care. A normal result does not rule cancer out, and they do not track new colon polyps, which is your main long-term consideration.
A question to bring to your next visit: "Are whole-body MRI or MCED blood tests worth it in my situation, or do my colonoscopy and routine follow-up already cover what matters most?"
Questions to decide together
These are framed as questions, grouped by timing, so you and your team can decide together.
- Is my next colonoscopy on the schedule for later in 2026, and what should I do if I have not received an appointment?
- My hemoglobin has climbed for over two years. Have we checked an EPO level, and would seeing a blood specialist make sense?
- My B12 has been high for a couple of years. Is that worth its own check?
- My A1c has gone up recently even on my current medicine. Would seeing a metabolism specialist help?
- After my 2026 colonoscopy, how often should I have them given my polyp history?
- Given my family history, are there other cancer screenings I should plan for?
- Would a ctDNA blood test add anything for me, or does it not address new polyps?
- Who should I list as my emergency contact and main support person?
Your CaringHand companion, anytime
Grace is available any time, day or night, to help you understand your plan and take small next steps. Grace explains and supports. Your care team makes the decisions.
- Answers your questions in plain language, like what a lab value or term means.
- Adds questions to your next-visit list so nothing gets forgotten when you see your doctor.
- Shares concerns with your care team when you want them to know something.
Grace is a support tool, not a substitute for your care team. If you ever experience thoughts of hurting yourself, call or text 988 or contact emergency services.
Explore at your own pace
Grace explains and supports. Your care team decides. You can ask Grace about any of these whenever you want.
Understanding long-term risk
You have said this is a priority for you.
Explain in plain terms what early-stage colon cancer and a polyp pattern mean ahead.
Any time you want your specific plan confirmed.
Family history & screening
Your family history can shape what screening makes sense.
Help organize your history and the questions to ask.
When deciding on added screening or genetic counseling.
Blood counts & B12
This is the item your team is most likely to look into next.
Explain what these numbers are and what a workup might involve.
To confirm whether and when to see a blood specialist.
Blood sugar & metabolism
Small steady improvements help your whole body, including your colon.
Explain your numbers and everyday supports.
For any change to your treatment.
Sleep
Good sleep-breathing support helps many other numbers.
Share tips for CPAP comfort and consistent sleep.
If sleep feels poor or your device feels off.
How you are feeling
Living with a cancer history and several conditions is a lot to carry. Your emotional health matters as much as the rest.
Offer a calm, private space to talk things through and help find support if you want it.
Any time, and especially if your mood changes.
Words explained simply
Underlined terms throughout this plan link down to here. You can also ask Grace to explain any of them.
This is a living document
It is only as good as the information behind it, so your input matters. Tell your CaringHand team or Grace if anything here needs fixing.
- Is anything in your story incorrect or out of date?
- Are any medications or diagnoses listed wrong, or is anything missing?
- What questions or worries would you most like Grace to help you with?
Clinical companion to the Living Action Plan
Clinical overview and staging
Malignancy arose within a tubulovillous adenoma; ~3 mm invasive focus, negative margins (~0.3 cm clearance), no lymphovascular invasion. Endoscopic hot snare polypectomy (2023); observation over segmental colectomy given low-risk features. Surveillance polypectomies in 2023 and 2025 (metachronous tubular adenoma, ascending colon; hyperplastic polyp, sigmoid). The metachronous adenoma across three procedures confirms a polyp-former phenotype (field effect), supporting a tighter than standard low-risk interval.
Molecular and genetic risk guideline
Germline testing on an expanded panel (>70 genes, including BRCA1/2, CHEK2, ATM, PALB2, NTHL1 and the Lynch MMR genes): negative. A negative broad panel reduces but does not eliminate familial risk. Family history is notable: father with colorectal cancer in his 50s and significant heart disease, paternal grandfather lung cancer, maternal uncle with a GI cancer in his 70s. Tumor MMR/MSI status is not documented; NCCN recommends universal MMR/MSI testing on colorectal tumors regardless of stage, so retrospective MMR/MSI IHC on the original specimen is reasonable to close the Lynch loop and inform family screening. Maintain a low threshold to revisit genetic counseling if new family events emerge.
Root-cause systems map hypothesis-generating
A multidisciplinary clinical review framed the survivorship picture as one network with several surface presentations. Modifiable upstream drivers converge on this member's dominant long-term risks (metachronous neoplasia and secondary erythrocytosis) more than on occult MRD.
Highest cross-system levers: break insulin resistance (endocrine tuning, resistance training), optimize OSA (CPAP adherence, sleep study recheck), inflammation modulation (Mediterranean pattern, omega-3), acid-suppression review, and a true hematology workup rather than a recheck. Concept figure is illustrative, not patient-specific imaging.
Hematologic concern: sustained erythrocytosis with elevated B12 workup indicated
Progressive Hgb 14.8 to 17.9 g/dL over ~2 years (Hct 51.2%), with B12 sustained >2000 pg/mL for about two years and coded "secondary polycythemia" and "other hemoglobinopathies." This pattern exceeds a 2-week recheck. Recommended workup: serum EPO; JAK2 V617F if EPO suppressed; hemoglobin electrophoresis; ferritin and iron studies; hematology consultation. Differential spans OSA-driven secondary erythrocytosis (primary hypothesis) versus a myeloproliferative process; hepatic steatosis can contribute to elevated B12.
Key labs and trends
Hemoglobin, g/dL (ref 13 to 17.7 M)
Sustained rise above reference. Hct 51.2%. Workup indicated.
A1c, % (target individualized)
Nadir 6.1 (mid-2025) then rise to 6.9 on tirzepatide 15 mg + empagliflozin 25 mg + metformin. Glycemic deterioration on max-tier therapy.
| Test | Latest | Reference | Trend / note |
|---|---|---|---|
| Hemoglobin | 17.9 g/dL | 13 to 17.7 (M) | Rising 2+ yr; Hct 51.2% |
| Vitamin B12 | >2000 pg/mL | 232 to 1245 | Sustained ~2 yr, no injectable B12 |
| A1c | 6.9% | 4.8 to 5.6 | Worsening on max therapy |
| Triglycerides | 265 mg/dL | <150 | Peak ~740 (2023) w/ pancreatitis hx |
| HDL | 34 mg/dL | ≥39 (M) | Chronically low for years |
| LDL | 51 mg/dL | <100 | At goal on simvastatin |
| Calcium | 10.3 mg/dL | 8.5 to 10.2 | Single, mild; PTH + 1,25-OH D pending |
| CEA | 1.8 ng/mL | 0 to 4.7 | Stable 1.3 to 1.8 over 3 yr |
| eGFR / creatinine | 112 / 0.68 | >60 / 0.7 to 1.3 | Low creatinine reflects low muscle mass |
Pharmacology and reconciliation
Active regimen (2026): metformin 1000 mg BID; tirzepatide 15 mg SC weekly (max); empagliflozin 25 mg daily; losartan 100 mg daily; amlodipine 5 mg daily; simvastatin 40 mg HS; famotidine 40 mg daily; omeprazole (dose to confirm); trazodone 50 mg HS; fluoxetine 20 mg daily; albuterol MDI PRN. Reconciliation: patient listed lisinopril (documented allergy, cough) likely confusing it with losartan; patient did not mention fluoxetine, omeprazole, or albuterol. Dual acid suppression is a deprescribing candidate pending symptom history. Note: SGLT2 inhibitors can modestly raise hematocrit via EPO and hemoconcentration, relevant to the erythrocytosis differential; any medication change is a prescriber decision.
Surveillance protocol and care-routing
| Item | Cadence / action | Owner | Timeline |
|---|---|---|---|
| Colonoscopy | Later in 2026, then q1 to 3 yr (polyp-former); HD scope reasonable | Onc / GI | On schedule |
| CEA | At oncology visits (stable trend) | Oncology | Routine |
| Routine CT | Not indicated for resected Stage I per NCCN | Oncology | n/a |
| Retrospective MMR/MSI IHC | On original specimen (Lynch completeness) | Pathology / Onc | ~4 weeks |
| Hematology referral | EPO; JAK2 if EPO suppressed; Hgb electrophoresis; ferritin/iron | PCP / Onc | ~4 weeks priority |
| Endocrinology referral | Glycemic optimization / combination tuning | PCP | ~3 months |
| PTH + 1,25-OH vitamin D | Characterize mild hypercalcemia | PCP | ~4 weeks |
| Sleep medicine | CPAP adherence download; study recheck given Hgb | PCP / Sleep | With heme workup |
| Medication reconciliation | Lisinopril vs losartan; fluoxetine, omeprazole, albuterol; dual acid suppression | PCP | Next visit |
| Problem-list cleanup | AFib, atypical angina, CHF, coronary atherosclerosis (clean recent CTA) | PCP | Next visit |
| Immunizations | Hep B and Hep A series (non-immune) | PCP | ~3 months |
Red flags and escalation
| Signal | Action |
|---|---|
| Hgb rising further or unexplained on recheck | Hematology consult, do not defer |
| Rising CEA trend | Oncology + PCP; consider imaging |
| New rectal bleeding, bowel-habit change, or weight loss | Earlier colonoscopy; do not attribute to hemorrhoids without visualization |
| Fasting glucose persistently >200 | Endocrine escalation; consider CGM |
| Triglycerides >500 | Pharmacologic therapy (icosapent ethyl or fibrate); pancreatitis risk |
| Calcium >11.0 on recheck | Evaluate for primary hyperparathyroidism |
| New family cancer (breast, GI, or under-50 onset) | Repeat genetic counseling |
| Mood change or suicidal ideation | Urgent psychiatric evaluation; 988 if crisis |
Evidence base
Evidence grade shown per item. Functional-medicine / systems framing is hypothesis-generating, not guideline-grade.
- NCCN Clinical Practice Guidelines in Oncology, Colon Cancer: surveillance and universal MMR/MSI testing. guideline
- Tefferi A, et al. Polycythemia vera. Leukemia 2021;35:3339-3351. guideline-adjacent
- Nguyen CD, Holty JC. OSA and secondary erythrocytosis. Respir Med 2017;130:27-34. evidence
- Stein KB, et al. Diabetes and colorectal cancer outcomes. Dig Dis Sci 2010;55:1839-1851. evidence
- Nakamura Y, et al. ctDNA molecular residual disease in resectable CRC. Nat Med 2024;30:3272-3283. evidence
- Campbell KL, et al. Exercise guidelines for cancer survivors. Med Sci Sports Exerc 2019;51:2375-2390. consensus
- Bhatt DL, et al. Icosapent ethyl for hypertriglyceridemia (REDUCE-IT). NEJM 2019;380:11-22. RCT
- Lindor NM, et al. Familial cancer susceptibility syndromes. JNCI Monogr 2008;(38):1-93. reference
Gaps, validation, and signoff
Critical gaps: EPO, JAK2 (if EPO suppressed), hemoglobin electrophoresis, status of the post-baseline recheck, full medication reconciliation. Important: PTH + 1,25-OH D, ferritin/iron, endocrine referral status, tumor MMR/MSI, 2025 colonoscopy pathology detail, CPAP adherence data. Conflicts: support-person discrepancy; lisinopril vs losartan; legacy cardiac codes vs clean recent CTA; non-disclosed depression/fluoxetine.
This is what your plan could look like
Every CaringHand member gets a Living Action Plan built from their records and reviewed by a licensed clinician, with Grace alongside to explain it any time.